
Frequently asked questions about Children and Youth Dentistry
Has your question not answered, then please contact us.
In the Canton Zug and in many communities of the neighboring cantons all children receive during compulsory schooling (ie from kindergarten entry) a voucher for an annual dental check with a dentist of their choice. Unfortunately, we note that in this age of the first visit to the dentist for many children is already "too late", it was because of any existing caries or because malocclusions that can no longer be covered by a supplementary insurance in this age. For these reasons, we recommend the first visit to the dentist as soon as possible, ideally at the first milk molar, but no later than before the 3rd birthday (age limit for many additional insurances). Thus your child can early get used to the dentist's office already. This first visit is mostly about information such as oral hygiene, misaligned teeth, Habits (pacifier, thumb, etc.), nutrition / feeding bottle etc. Last but not least we can so early build a trusting relationship with your child, what is very impotant for the future "dentist experience ". If a child is the first time visiting a dentist because of toothache, the visit from the outset has negative connotations and the construction of a foundation of trust is correspondingly difficult.
Dental visits are for some a completely normal thing. For others, it unfortunately still means just panic attacks, that often have their origin in bad childhood experiences at the dentist. We want to do everything possible to spare your child a bad experience, so that it can feel comfortable and build up confidence in "his/her" dentist. Good preparation of the child by your side is also very important and it can help us enormously with the following tips:
- Express yourself to your child always positive about the visit to the dentist
- Motivate your child positive by reporting experiences about the upcoming visit and also about your own (only positive ones!). Tell your child that we explain everything and show everything, and above all, that we look forward to meet you and your child.
- Convey your child never your own fears and unpleasant experiences
- Avoid threats ("because you do not brush your teeth, you have now to go to the dentist") or false promises ("it takes only 5 minutes at the dentist")
- Avoid soothing intentioned words such as
- You need to have no fear -> Your child hears only "fear"
- It will not hurt -> Your child hears only "hurt"
- That's not bad -> Your child hears only "bad"
- Please promise no reward gifts!
- This may sound a little hard, but this can potentially tremendously strengthen a pre-existing anxiety. Especially when it comes to things that your child heartfelt wishes, you will put your child under enormous pressure and making it difficult for us to work with your child. But after the appointment, you should absolutely commendable your child, what strengthens the self-confidence and motivation. There is also in our practice for each child a small gift for friendship, that will never just depending on a successful treatment.
For the first visit, we take a lot of time for the child to make it playfully used to the new situation and it can build confidence in the practice team. Our first meeting we would only use for a personal interview and a exact examination and diagnosis. For an accurate diagnosis, we need an accurate clinical examination of the teeth and mouthcavity. Possibly also the production of X-ray images is necessary. In this first appointment no treatment is taking place, but further action and the right type of treatment will be discussed with you and your child.
In a healthy dentition an annual check is sufficient. Further dates or controls must be arranged individually, depending on whether prophylactic or conservative treatments are necessary. Depending on the level of development status it may also be, that a semi-annual inspection is advisable.
Caries is mostly being built in deciduous teeth "in the interdental spaces", which means to the surfaces on which two teeth touch each other. In the early stages this caries can only be seen on radiographs. Only when the caries is so far advanced, that a part of the tooth erupts, the caries is clinically directly visible. For this reason, we recommend already on suspicion of caries or tooth decay to make individual teeth x-rays for an accurate diagnosis. Various studies confirm that routine radiological monitoring at the age of approximately 6 years and 12 years is reasonable. In caries risk patients we recommend radiological monitoring at least every 2 years. In addition, other incidental findings on radiographs are seen as agenesis, tooth misalignments, cysts etc. The timely knowledge of such changes gives us time to evaluate the according necessary actions.
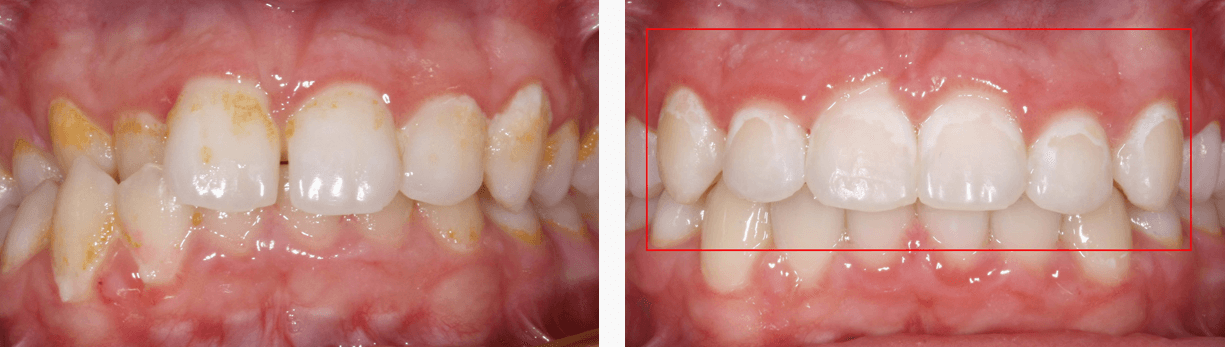
Caries is an infectious disease, according to the World Health Organization (WHO), even the most prevalented worldwide. Almost 95% of the population are affected. Caries, as also indeed gum diseases, are caused by bacteria. To suffer from tooth decay, you have to be infected first with these bacteria. This is unfortunately inevitable. A newborn is not yet colonized by cariogenic bacteria, but the initial infection takes place mostly already in infancy through saliva contact (licking the spoon, pacifier or by parents kissing, coughing, joint use of dishes, etc. with their kids). The Parents caries-causing bacteria colonize also the oral cavity of the child. You can avoid a transfer hardly, which would be illusory. However, is not disputed, that the subsequent decay rate is higher, the earlier the infection with caries bacteria happens. Children, who were infected at a very early years of their life, got caries 89% before the age of 5 (Source: Chlorhexamed®). Thus we are all carriers of this disease, it is a matter of time and above all the correct individual prophylaxis, whether, how and how often the disease breaks out. The aim is to keep the number of bacteria always as low as possible (keyword: good oral hygiene) and the bacteria not to offer a possible substrate (keyword: sugar intake). The bacteria convert existing carbohydrates to acid, which attacks the tooth structure and this leads in the long term to tooth decay. This is called demineralization of the tooth. As long as the demineralization is limited to the melt (so-called white spots), it is reversible by appropriate actions (professional oral hygiene, intensive fluoridation). Once the demineralization reaches the dentin, the tooth can be only repaired by removing the diseased parts and replacing the loss of substance with a filling. This repairs, compared to the original tooth material, are limited in time as well as everywhere in life. If no repair takes place, the caries will continue to progress towards the pulp (nerve cave), which then results in pain and inflammation, as well as a much more expensive root canal treatment. In the worst case, the tooth must be completely drawn out.

Before with oral hygiene already bad at the beginning and afterwards with oral hygiene always bad during treatment.
It has to be cleand from the first tooth! It sounds simple and it is logical - if it were not for the strong will of the little person, who belongs to this tooth ... Do not be insecure, if your child refuses to brush your teeth. You don't him any favors if you give up. Once the first milk tooth can be seen (about 6-9 months), it should be 1x daily cleaned with a fluoride children's toothpaste (ideally in the evening after the last food intake). This is important, because the teeth are not fully developed during the breakthrough and particularly susceptible to dental caries. The best way for your baby to get used to the toothbrush to is even before the first tooth appears. It can playfully put it in its mouth and so it can explore in peace and will not be so suddenly "invaded". Rule of thumb for cleaning: the 1st year of life 1x daily (evening), in the 2nd year of life 2x daily (morning and evening) and from 3rd year 3 times a day (morning, noon and evening). May until the child spit out correctly, we recommend the children's toothpaste, which has a much lower fluoride content than adult toothpaste. Once the child can spit out well and at the latest after the eruption of the first permanent teeth, it should necessarily be changed on a junior or adult toothpaste. We also recommend, that from then also the use of fluoride gelée 1x a week to additionally build the acid resistance of the new teeth. What toothpaste brand is used is completely beside the point. It is important, that your child likes to use the toothpaste. Because even the mot expensive toothpaste is useless, if it is just in the cupboard. After brushing, your teeth should not be rinsed with water, to spit out the toothpaste is completely enough, so that fluorides may act longer after. You should also up about 8/9-year at least 1x a day (preferably at night) control and help your child with brushing its teeth. Generally, it plays less of a role as often the teeth are cleaned, but rather how thoroughly. Especially dental hygiene in the evening is of utmost importance, since our body at night produces many times less saliva than during the day, which represents an additional safety mechanism for the teeth. This is also one reason why "giving the bottle" at night is so terribly harmful to the teeth. In conclusion remains to be mentioned, that you should also paid attention to the appropriate toothbrush. There are now different sizes depending on their age, it is important here that an appropriate size is chosen and the brush has soft bristles (the same also for adults: hard bristles clean not thorough, but scratch the tooth surface resulting in faster discoloration and are very harmful for the gums!). The question whether electric or manual toothbrush is better: our prophylaxis assistant can individually give you the best advice by an appointment with her. If electric then definitely a sonic toothbrush and not arotating one (round brush head). In addition, children should themselves at first learn the correct handling of the hand brush. For subsequent cleaning by the parents an electric toothbrush, however, can be a tremendous help.
There are many children, who will not brush their teeth the first years of life. Before you give it up, go and get advice from your dental practice! We will gladly support you and most of us can draw from their own experience. The most important thing for you is to know, you don't hurt your resisting, when you brush its teeth (it costs nerves, but this applies also to other situations in life with kids ...). But if you let it be, your child will in the long run have very big problems and sooner or later also usually pain.
Fluorides remain stable in an acidic medium, therefore cause the milieu the caries bacteria through the breakdown of carbohydrates. They are installed in the enamel and form a protective layer of fluoride apatite, which protects the tooth from further demineralization. So fluoride increases the chemical resistance of the tooth and supports the repair mechanism (remineralization). This repair mechanism can only take place, if the bacterial plaque will be removed regularly on the teeth.
When sugar (generally in carbohydrates), it is unfortunately so, that it does not depend so much on the quantity, but especially on the frequency how often per day sweet (also hidden sugars!) is consumed. The caries bacteria convert the carbohydrates into acids, leading to demineralization of the dental enamel. Does a child therefore drink regularly several times a day highly diluted fruit juice or syrup (worst yet permanently sucking on the feeding bottle), this is even much more harmful than if it per day (to eat) takes once a more sugary drink. In the first case the environment in the oral cavity is almost permanently sour, in the second case only during the meal. By the normally following brushing, the remineralization is initiated.
Below are some tips for dealing with sweets:
- Forbid your child no sweets, prohibitions are particularly interesting and only lead to the fact, that the children get the sweets elsewhere and you have no control over it.
- Set rules! For example no such sweet before eating (sweets should not be a substitute for a meal). If your child gets sweets from many sides (grandparents, godfather, the nice lady at the grocery store, etc.), place with him a candy treasure chest in which it can keep its treasures, and it may snacking for example, in the evening a little after dinner, but before brushing.
- Go by yourself with a good example ahead!
- Watch out for hidden sugars, read the ingredients list. Especially in ready meals and so-called "children's foods" (Milchschnitte, Carpi-Sonne etc.). Those ingredients that are most included, are on the first 3 digits in the composition.
- An alternative to Bubblegum, Lollipop and Co. are tooth-friendly sweets. You can identify these at the sign with the "Happy Tooth under the umbrella"
Milk teeth are the first teeth and fall out some day. But they are of different length in the mouth (the front teeth begin about 6-7 years to change, the rearmost until about 11-13 years), and they assume at this time very important functions (eating, language training, jaw growth, place holder for the following permanent teeth). Not treating carious in primary teeth usually leads to pain and abscesses (which can be very dangerous, however, and they can spread via the blood throughout the body and all organs). By caries caused too early tooth loss can lead to stunted growth and lack of space, which can cause later higher orthodontic costs and generally more difficult orthodontic treatment. If the teeth are so severely damaged, that they must be removed at an early stage, we recommend the lateral teeth (molars) urgently needed a place holder to prevent developmental disabilities and loss of space.
If the caries progressed to the tooth nerve, it reacts with a strong inflammation. This caused damage throughout the tooth root and also in the surrounding tissue and bone. A thick jcheek often indicates an accumulation of pus. Here it is very important as soon as possible to treat the cause, ie to remove the infected tooth to prevent further spread and damage to the underlying tooth germ.

In acute inflammation, we reach with a local anesthetic no pain relief, because the painkiller does not act in this situation. In addition, the child is usually not treatable at this moment because of the ongoing severe pain. In this case, we prescribe antibiotics to relieve acute inflammation and to create appropriate conditions, so that we can treat your child as painless as possible. Antibiotic treatment is for about 7 days, then normally the removal of the tooth can be done with a normal local anesthetic. Sporadic toothache (sometimes more, sometimes less) can briefly be treated with common painkillers (Algifor, Dafalgan, Voltaren). Here, however, it is merely symptomatic treatment to briging the pain phases for a short time. Adequate treatment of the cause should be done by the dentiste as quickly as possible.
Tooth decay is always a lengthy process, but can initially run very hidden. In particular, the contact surfaces of the teeth ("interdental spaces") are clinically accurate examinable neither for you as parents or for us as professionals. For this reason, we recommend, that in case of suspicion or of a certain age as a routine check, to make X-ray images, in order to examine precisely these areas in more detail and to detect any caries as early as possible. If a defect arises in such a place, the "hole" grows in the beginning larger against the tooth inside. Over time, the surface is then so weakened by the lateral hole, that part of the tooth breaks off. At this moment, then suddenly a big hole will appear, which should be treated with as quickly as possible.
The teeth, which are at erupting through the gums, are still very vulnerable to acid, because their surface is not fully developed yet. Thus the surface already will be damaged during the dental eruption by bacteria and frequent sugar intake. Particularly common seen here is the form of the so-called "Bottle caries", which means that sugary drinks (so-called Child-Tea, milk powder bottle, but also dilute fruit juices, syrups, chocolate milk, etc.) are given in the feeding bottle, unfortunately often when falling asleep or during the night. The teeth were healthy, as long as they were not in the oral cavity, but were attacked there and destroyed immediately. That is why it is so important to pay attention to the correct content of the feeding bottle (milk or water) and to clean the teeth after sugary bottle-meals and never to give the bottle to calm down the child, to fall asleep or even at night at bed. In addition, the child should be encouraged from 1 years old to drink from a cup, as long sucking on baby bottle or pacifier has a harmful effect on the jaw development.
Caries is an infectious disease. The onset of the disease, so the development of dental caries, is not hereditary. The infection can, however, take place early depending on the habits. Then even more bad "familiar-traditional" habits regarding bad nutrition and oral hygiene are continued, this will lead inevitably to caries...
There are at least as many dental insurance as insurance providers, therefore this question is not easily to answer yes or no. It depends very much on what you expect from your insurance, which costs are to be covered in case of an emergency and what cases can happen. In the so-called dental care insurances annual inspections are mostly covered (which are indeed already paid by the municipality by the school-voucher), as well as prophylactic measures, such as dental cleanings and - depending on the insurance contributions - to certain other dental procedures (tooth renovations). However, these vary considerably. Depending on the risk of tooth decay, such a insurance can really make sense. In generally an insurance for orthodontic treatments can be of advantage, since these are often necessary (misaligned teeth, as opposed to tooth decay, are really inheritable, which means if you as father or mother have already passed through an orthodontic treatment, it is also lies your child ahead with high probability). It is important to know, that an insurance can not be completed, if misalignments or treatment is already visible! This is particularly important, if you consider a possible insurance change. Most insurers already request very early (from 3 years) a corresponding dental certificate, that certifies that everything is order.
The sooner the better! Sucking can cause misalignments of jaw and teeth as well as malfunctions of the soft tissues (tongue, cheek). Pacifier or soother can be used without a problem till the end of the second year. But from the 2nd birthday, you should gradually begin to get out of the habit (only to calm down/ for falling asleep). Should the child after the 4th birthday still hang on his pacifier / thumbs, we can advise you individually, how to get your child out of this habit.
The molars have grooves and pits on the chewing surfaces, so-called fissures. For some people these fissures are relatively flat, for others very deep and hardly to clean properly with a toothbrush (this applies especially frequently to the first permanent molars). Bacteria can penetrate into these deep pits and so lead to tooth decay, so they can not be removed with normal oral hygiene. In these cases we recommend a fissure to prevent decay. The caverns are thoroughly cleaned by us and then so far filled with a runny white composite, that good cleaning conditions can be established. As a rule, these are a one-off treatment, in rare cases, the seal needs to be replaced after some time. Important are the right conditions to ensure a good seal, ie. the tooth must be completely broken through in order to have appropriate dry conditions and the child must join good for treating. A sealant is absolutely painless, we explain to the children, that it is a principle similar to paint fingernails.
Unfortunately, until today there is no such protection film, which can be pulled over the teeth. When we talk about sealing, we always mean the pits in the teeth, unfortunately the remaining surface can not be treated, the material would not hold and certain surfaces (contact surfaces of the teeth) could be reached because of anatomical and technical reasons.
A steel crown is a prefabricated crown of stainless steel, which is used for heavily damaged milk molars. If not enough tooth structure for a white filling (composite) is present, we can create good conditions with the steel crown, so the affected tooth can remain in the mouth until it naturally fails out. The crowns are silvery, since they are made of stainless steel. This makes them very well tolerated and the crown can be adjusted individually to the respective tooth. The acceptance of children for such "knights teeth" is very good in general. There are also stainless steel crowns, which are blinded with a white ceramic layer, this can not, however, adapted to the tooth, also the white material fragmented quickly, whereby the treated teeth very soon no longer look beautiful. The latest generation are white porcelain crowns, which we do not yet offer especially for reasons of costs.

A placeholder is a kind of "mini braces". When a milk molar tooth has to be removed to early, a placeholder is used to keep the resulting gap open until the new permanent tooth erupts. The most efficient placeholders are cemented laboratory fabricated and fixed on one or two adjacent teeth. When the permanent tooth erupts, the placeholders can easily be removed again.

The nitrous oxide treatment is a so-called "inhalationssedation", so a treatment with a sedative (strong sedative) via the breathing is supplied to the body. It's not magic, even though many want to believe, and we explain the smaller children the treatment as "magic air". But nitrous oxide can help anxious children to open up for a treatment and to feel calm and relaxed. Nevertheless, we have to rely on this form of treatment on a basic compliance of the child. A great advantage is also, that the nitrous oxide is absorbed directly via the lungs and is not metabolized in the body. Once the nitrous oxide supply is interrupted and the sedative effect stops. Thus, the children can leave the office immediately after the treatment. However, we recommend not to leave the children alone directly on the road or to visit immediately after a gymnastics or swimming lesson.
For nitrous oxide treatment, we need a fundamental treatment readiness of the child so far, that the child can put on a nasal mask and is able to breath with closed and open mouth through the nose. If the child already this refuses, no treatment is notabene possible with nitrous oxide. Otherwise, there are children, who respond very well to the inhalationssedation and the necessary treatments can be so easily carried out. But there are also children, who indeed the sedation acts superficially, but is not yet sufficient for larger treatments. This is true in very young children (3-6 years), who at the same time need a very large treatment.
Nitrous oxide is a sedative, not an analgetic, so it can not eliminate or affect the perception of pain. For this reason, in prospectively painful procedures (including most dental treatments) an additional local anesthesia is necessary. Note, however, that we look out in our work with children in general on a child-friendly language, and avoid words, that seem scary from the outset!
Under general anesthesia, the child is asleep and gets from treatment anything with. Such treatments are necessary for extensive dental procedures, if no cooperation from the child based on age / groth can be expected or sometimes even with very painful procedures, where a local anesthetic alone is not sufficient. The treatment is performed on an ambulant basis, which means that the child about 1 hour after the treatment may leave the practice again. Treatments under general anesthesia can be performed directly in our office. The general anesthesia itself is always performed by certified professionals (anesthetist and nurses) and so also be invoiced separately. The cost of an general anesthetic treatment are normally not covered by the basic health insurance.
Dental treatments generally are not covered by the basic health insurance, thus also the cost for the general anesthesia caused of a dental treatment are not covered by the basic health insurance. If you may have a additional insurance for dental treatment, it really can be, that the costs are covered. The best thing will be, if you ask your insurance consultant before the treatment.
In most municipals a dental check up is obligatory, if you child reaches the compulsory school attendance age (Kindergarden). The implementation of the annual check up varies widely. In some communities the check up will carried out within a school dental clinic ("Schulzahnklinik") , elsewhere the children receive vouchers, that you can redeem at a dentist of your choice or in some municipals only with certain dentist or there are also communities, who don't pay for it at all.
In our practice, the annual check-ups are uniformly organized. The annual dental check-up consists of a clinical inspection and a short tooth cleaning for removal of the biofilm (bacteria coating) including fluoridation of the teeth. Since the vouchers vary greatly in their value, we charge our services and deduct the voucher value on our invoice. Thus, we can almost redeem every voucher you hand in. Please remember to bring your voucher with you to the appointment and give it to your receptionist before the treatment.
First, it depends on the severity of the accident, in particular whether other serious head injuries took place. Is the child conscious? Does your child suffer from dizziness / headache / nausea / vomiting (indications of a concussion) or did more major injuries happen (cuts / breaks / open injuries)? Such injuries always require a primary care by the emergency doctor or the hospital!
Furthermore, the age of your child and thus the affected teeth play a role. Are baby teeth or permanent teeth involved? If a tooth is displaced, smashed, knocked out or broken? Does it bleed? From the soft tissues (lips, gums, tongue) or from the tooth? Please find first recommendations on how quickly you should see a dentist and how to deal with knocked out teeth in a dental accident brochure down below.
Rule of thumb: If permanent teeth are affected, see a dentist as soon as possible (immediately). Are baby teeth injured, it rather depends on the extent of the injury. Do not try to insert knocked out baby teeth back in place as the permanent tooth germ can be damaged. With displaced baby teeth: try to align them into their original position within 1 hours after the accident, so that your child can bite normally. To achieve that, you can use your finger or a pacifier/dummy. If the tooth is blocked and can not been replaced, the dentist may still try to solve the blockage (usually it is a fracture of tooth-bearing bones), but only when the treatment can be carried out within the next 1-2 hours. An immediate visit to the dentist is also recommended, if the deciduous teeth accident includes bleeding either from the soft tissues or from the tooth. The same is also true for falls on the chin (possible condyle fracture of mandible), especially if the bite shifted and the child can not close as before. If only a small corner of a milk tooth is broken and the child has no major complaints, a check up with the dentist is recommended within a few days. Nevertheless, an examination with the dentist and a filling of claim with the accident insurance is advised, so that further later treatment will be covered by the insurance.

